
I
Tepkinly is licensed
for 3L+ DLBCL
Tepkinly as monotherapy is indicated for the treatment of adult patients with relapsed or refractory diffuse large B‑cell lymphoma (DLBCL) after two or more lines of systemic therapy.1
Tepkinly has a conditional marketing authorisation
- further data awaited.
You are advised to read the Prescribing Information and Summary of Product Characteristics, accessible via the links above, to evaluate patient suitability for Tepkinly.
Adverse event reporting information can be found at the bottom of this page.

Tepkinly is licensed for 3L+ DLBCL
Tepkinly as monotherapy is indicated for the treatment of adult patients with relapsed or refractory diffuse large B‑cell lymphoma (DLBCL) after two or more lines of systemic therapy.1
Tepkinly has a conditional marketing authorisation
- further data awaited.
You are advised to read the Prescribing Information and Summary of Product Characteristics, accessible via the links above, to evaluate patient suitability for Tepkinly.
Adverse event reporting information can be found at the bottom of this page.

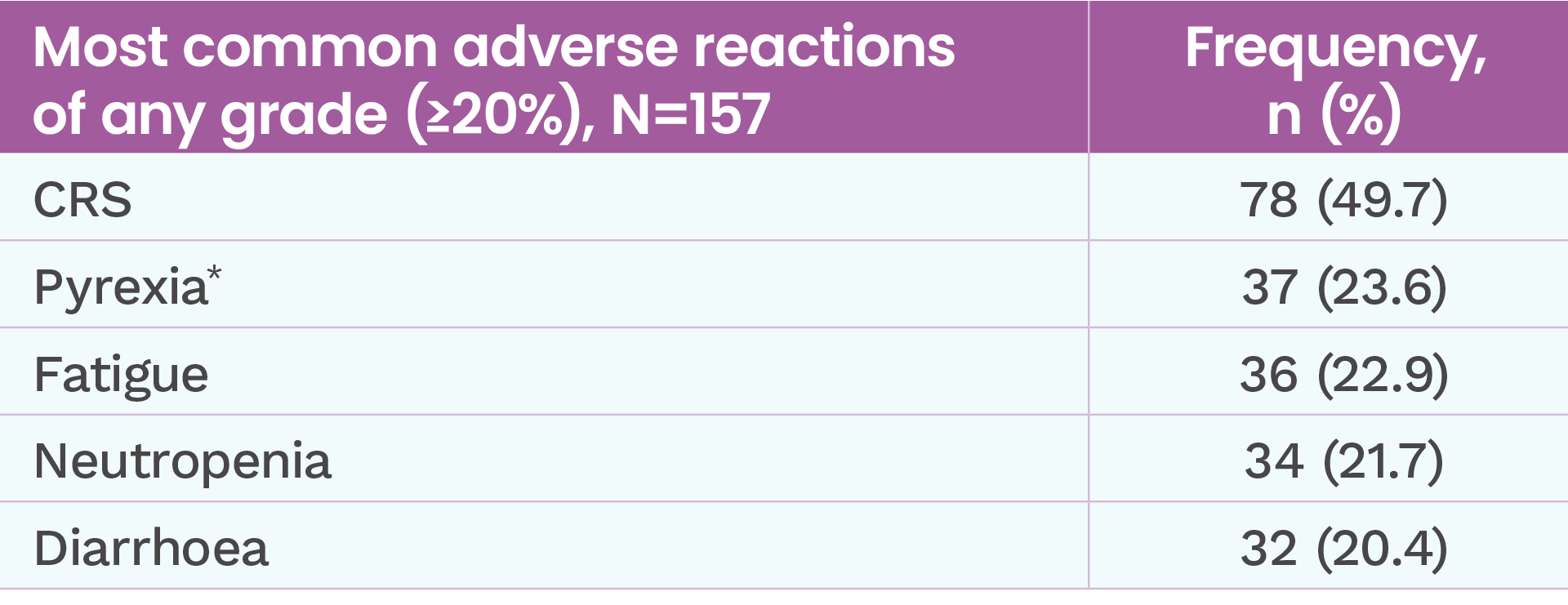
Adverse reactions reported in patients in EPCORETM NHL-12
The safety of Tepkinly was evaluated in a non-randomised, single-arm study in 157 patients with relapsed or refractory LBCL after two or more lines of systemic therapy and included all the patients who received at least one dose of Tepkinly.1
For full safety information, please refer to the NI SmPC (www.emcmedicines.com/en-gb/northernireland/)
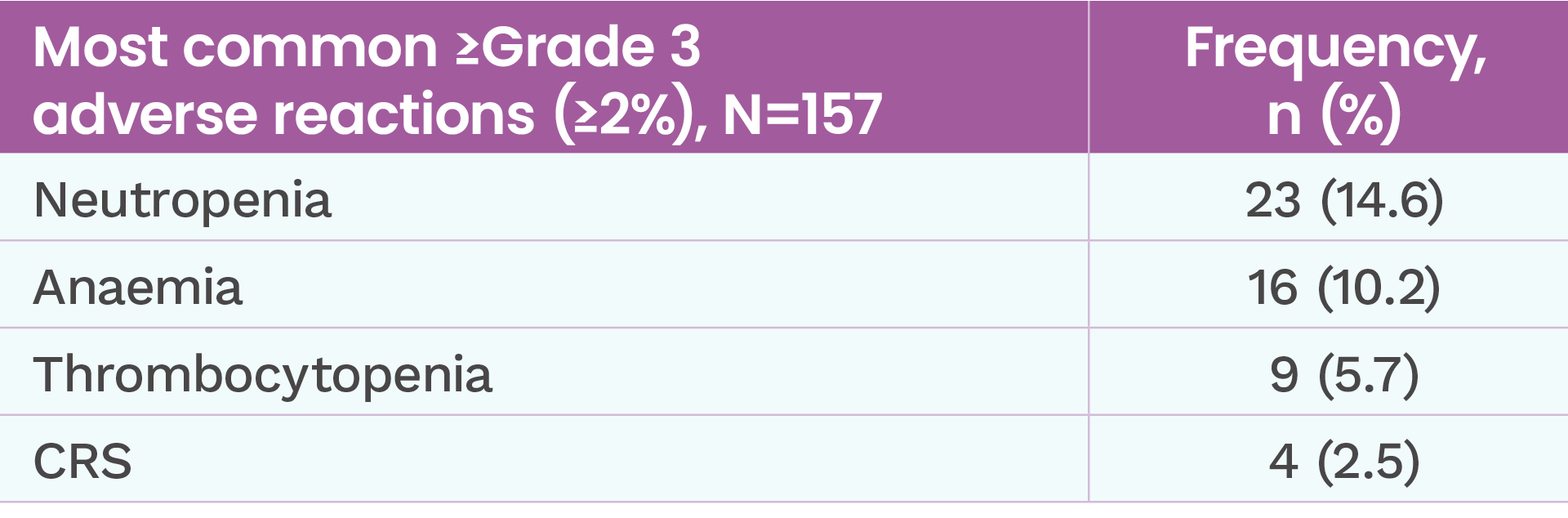
- Serious adverse reactions occurred in 56.7% (n=89/157) of patients.
- 5.7% (n=9/157) of patients experienced a fatal treatment-emergent AE (COVID-19 in 1.3% (n=2/157) of patients and myocardial infarction, hepatotoxicity, progressive multifocal leukoencephalopathy, loss of consciousness, general health deterioration, pulmonary embolism, and ICANS in 0.6% (n=1/157) of patients each). Only the fatal ICANS event was considered related to Tepkinly.
Tepkinly has a generally manageable safety profile2
- 7.6% (n=12/157) of patients discontinued subcutaneous Tepkinly due to treatment-emergent AEs of any grade2


CRS events in the EPCORETM NHL-1 trial2
CRS of any grade occurred in 50% (n=78/157) patients treated with Tepkinly2
Predictable: Most CRS events occurred in Cycle 1 and were associated with the first full dose of Tepkinly2
- Median time to onset after first full dose was 20 hours
CRS events in NHL-1 trial by dosing period (full cohort, N=157)2
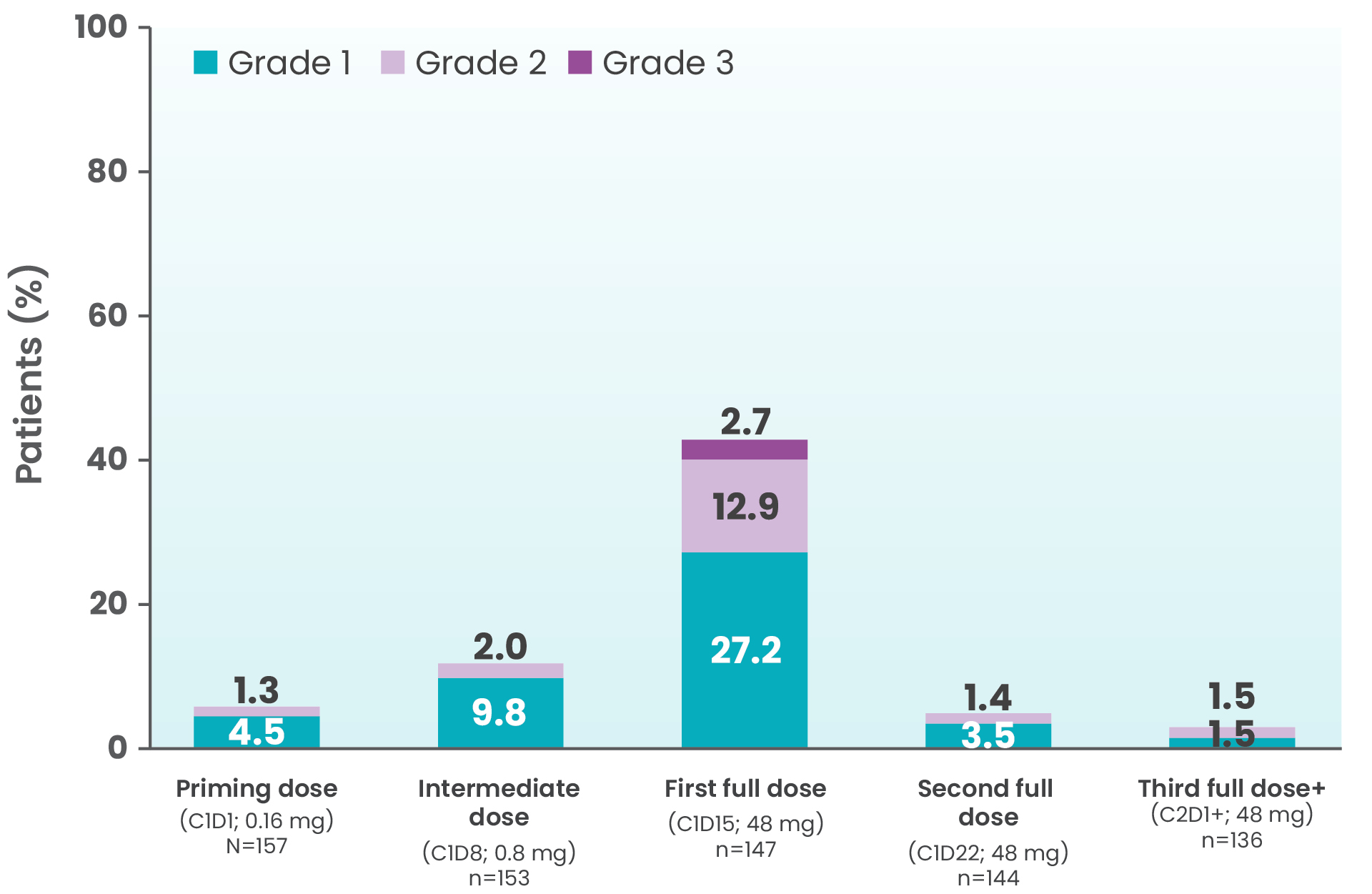
Manageable: Treatment was discontinued in 0.6% (n=1/157) of patients due to CRS2
Resolvable: CRS resolved in 99% (n=77/78) of patients2
- Median time to resolution from onset after first full dose was 2 days
Patients should be monitored for signs and symptoms of CRS following Tepkinly administration. Patients should be hospitalised for 24 hours after administration of the Cycle 1 Day 15 dose of 48 mg to monitor for signs and symptoms of CRS1
CRS was generally low grade2

Management of CRS while using Tepkinly1
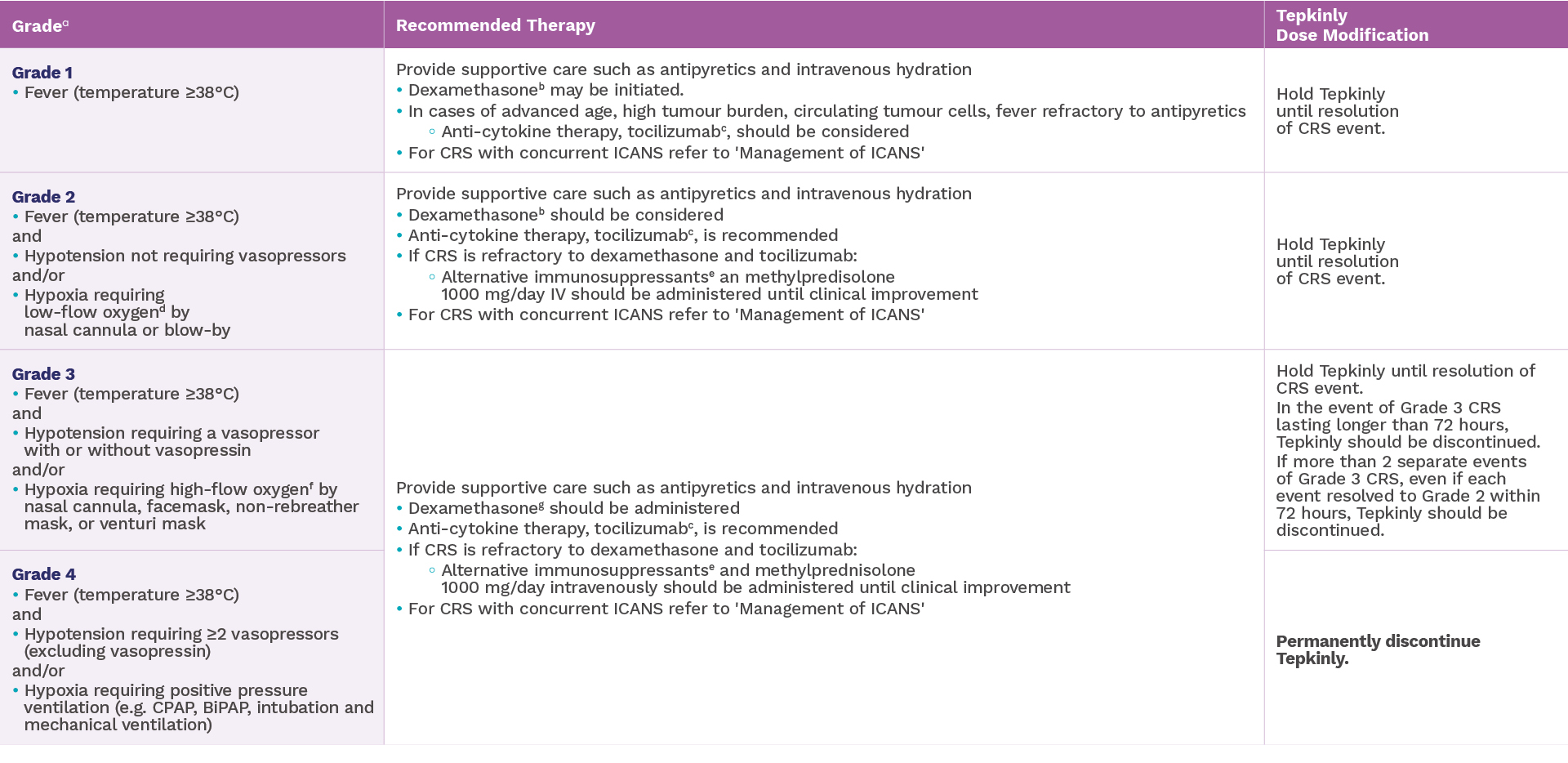
bDexamethasone should be administered at 10-20 mg per day (or equivalent).
cTocilizumab 8 mg/kg intravenously over 1 hour (not to exceed 800 mg per dose). Repeat tocilizumab after at least 8 hours as needed. Maximum of 2 doses in a 24-hour period.
gDexamethasone should be administered at 10-20 mg intravenously every 6 hours.
See bottom of this page for other footnotes.
ICANS occurrence in EPCORE™ NHL-1 trial2
ICANS occurred in 6% (n=10/157) of patients2
Frequency of ICANS by grade

- ICANS resolved in 90% (n=9/10) of patients with supportive care2
Patients should be monitored for signs and symptoms of ICANS following Tepkinly administration. Patients should be hospitalised for 24 hours after administration of the Cycle 1 Day 15 dose of 48 mg to monitor for signs and symptoms of ICANS1

Management of ICANS while using Tepkinly1
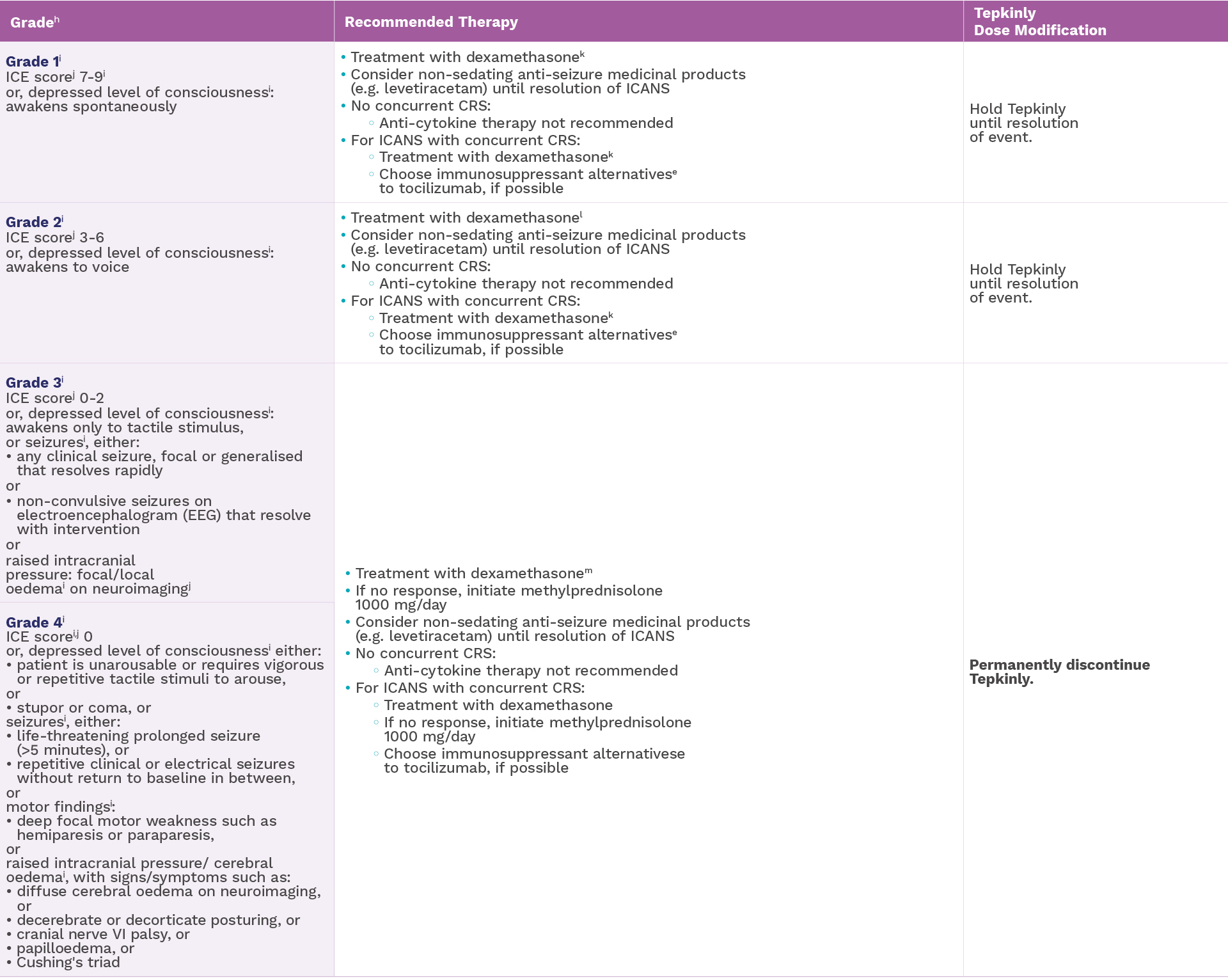
kDexamethasone should be administered at 10 mg intravenously every 12 hours.
lDexamethasone 10-20 mg intravenously every 12 hours.
mDexamethasone 10-20 mg intravenously every 6 hours.
See bottom of this page for other footnotes.
Serious infections of any grade occurred in 25% (n=41/167) of patients treated with Tepkinly1
- The most frequent serious infections were COVID-19, COVID-19 pneumonia, pneumonia, sepsis, cellulitis, upper respiratory tract infection, bacteraemia, septic shock and progressive multifocal leukoencephalopathy#
Frequency of serious infections

Fatal serious infections occurred in 7 patients (4.2%)
- Median time to onset of first serious infection from start of epcoritamab treatment was 56 days (range: 4-631 days)
- Median duration of serious infection was 15 days (range 4-125 days)
- Fatal infections (Grade 5) occurred in 4.2% (n=7/167) of patients
Administration of Tepkinly should be avoided in patients with clinically significant active systemic infections.
- As appropriate, prophylactic antimicrobials should be administered prior to and during treatment with Tepkinly.
- Patients should be monitored for signs and symptoms of infection before and after Tepkinly administration, and treated appropriately.
- In the event of febrile neutropenia, patients should be evaluated for infection and managed with antibiotics, fluids and other supportive care, according to local guidelines.
Recommended dosage modifications for adverse reactions other than ICANS and CRS1

**Based on National Cancer Institute Common Terminology Criteria for Adverse Events.
*Pyrexia not considered CRS by the investigator.
†Classified using MedDRA version 24.1. CRS events and ICANS events were graded per Lee et al; clinical tumor lysis syndrome was graded per Cairo-Bishop criteria. All other events were graded per National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.3,4
‡24 patients had CRS that was a maximum of grade 2 in severity; of these, 19 patients had hypotension, including 6 with concurrent hypoxia and 13 without concurrent hypoxia, and did not receive vasopressor treatment.
§One fatal case of ICANS was reported.
¶One patient (0.6%) experienced a fatal adverse reaction (ICANS).2
#Actual EPCORE™ NHL-1 study start date: June 26, 2018. Estimated Primary Completion Date: January 2025.5
aCRS graded according to ASTCT consensus criteria.
bDexamethasone should be administered at 10-20 mg per day (or equivalent).
cTocilizumab 8 mg/kg intravenously over 1 hour (not to exceed 800 mg per dose). Repeat tocilizumab after at least 8 hours as needed. Maximum of 2 doses in a 24-hour period.
dLow-flow oxygen is defined as oxygen delivered at < 6 L/minute.
eRiegler L et al. (2019).
fHigh-flow oxygen is defined as oxygen delivered at ≥ 6 L/minute.
gDexamethasone should be administered at 10-20 mg intravenously every 6 hours.
hICANS graded according to ASTCT ICANS Consensus Grading.
iICANS grade is determined by the most severe event (ICE score, level of consciousness, seizures, motor findings, raised ICP/cerebral oedema) not attributable to any other cause.
jIf patient is arousable and able to perform Immune Effector Cell-Associated Encephalopathy (ICE) Assessment, assess: Orientation (oriented to year, month, city, hospital = 4 points); Naming (name 3 objects, e.g. point to clock, pen, button = 3 points); Following Commands (e.g. “show me 2 fingers” or “close your eyes and stick out your tongue” = 1 point); Writing (ability to write a standard sentence = 1 point); and Attention (count backwards from 100 by ten = 1 point). If patient is unarousable and unable to perform ICE Assessment (Grade 4 ICANS) = 0 points.
kDexamethasone should be administered at 10 mg intravenously every 12 hours.
lDexamethasone 10-20 mg intravenously every 12 hours.
mDexamethasone 10-20 mg intravenously every 6 hours.
Abbreviations
ASTCT=American Society for Transplantation and Cellular Therapy; BiPAP=bilevel positive airway pressure; C1D1=cycle 1, day 1; C1D8=cycle 1, day 8; C1D15=cycle 1, day 15; C1D22=cycle 1, day 22; C2D1+=cycle 2, days 1+; CPAP=continuous positive airway pressure; CRS=cytokine release syndrome; DLBCL=diffuse large B-cell lymphoma; ICANS=immune effector cell-associated neurotoxicity syndrome; ICE=immune effector cellassociated encephalopathy; ICP=intracranial pressure; IV=intravenous; MedDRA=Medical Dictionary for Regulatory Activities; NHL=non-Hodgkin lymphoma; SI=serious infection; TLS=tumour lysis syndrome.
UK-EPCOR-240325. Date of preparation: October 2024.
Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk.
Adverse events should also be reported to AbbVie on GBPV@abbvie.com
